 You are, of course, aware that smoking can speed up the normal aging process of your skin, contributing to wrinkles.
You are, of course, aware that smoking can speed up the normal aging process of your skin, contributing to wrinkles. How does smoking lead to wrinkles?
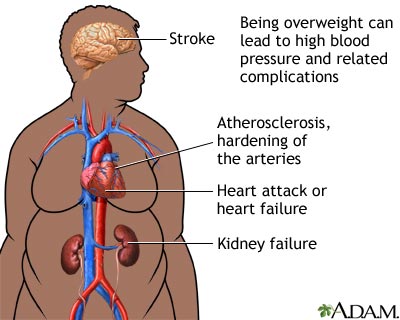
The nicotine in cigarettes causes narrowing of the blood vessels in the outermost layers of your skin. This impairs blood flow to your skin. With less blood flow, your skin doesn't get as much oxygen and important nutrients, such as vitamin A. Many of the over 4,000 chemicals in tobacco smoke also damage collagen and elastin, which are fibers that give your skin its strength and elasticity. As a result, skin begins to sag and wrinkle prematurely because of smoking.
In addition, repeated exposure to the heat from burning cigarettes and the facial expressions you make when smoking — such as pursing your lips when inhaling and squinting your eyes to keep out smoke — may contribute to wrinkles.
Smoking Also Causes PIMPLES!
Now, if yo u need another reason to motivate you to quit smoking, add pimples to the list.
u need another reason to motivate you to quit smoking, add pimples to the list.
Bruno Capitanio, M.D., of the Istituti Fisioterapici Ospitalieri in Rome, and colleagues examined 226 adult women with acne and found that 192 of the women (85 percent) had CPAA, and 34 had papulopustular postadolescent acne. One hundred fifty of the women (66.3 percent) were smokers, but smoking was identified in 72.9 percent of those with CPAA and only 29.4 percent of those with papulopustular postadolescent acne.
CPAA is comedonal postadolescent acne and it appears to be strongly linked to smoking cigarettes.
Nicotine is an agonist of acetylcholine (ACh) and it is thought that stimulation of ACh receptors on epidermal keratinocytes results in hyperproliferation and increased differentiation. To put it simply, nicotine causes the overproduction of skin cells which are shed more rapidly and then sticking together to plug the opening of the hair follicle. Sometimes the plugged hair follicles rupture leading to the formation of pustules, nodules, abscesses and cysts.
References
Capitanio B, Sinagra JL, Bordignon V, Cordiali Fei P, Picardo M, Zouboulis CC. Underestimated clinical features of postadolescent acne. J Am Acad Dermatol. 2010 Nov;63(5):782-8.
Acetylcholine: A key chemical in neurons (nerve cells) that acts as a neurotransmitter and carries information across the synaptic cleft, the space between two nerve cells.
Picture Credit 1; Picture Credit 2
CLICK HERE for more than 25 posts on Smoking Cessation.


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}